That sharp, aching pain in your shoulder when you reach for a coffee mug or try to sleep on your side is more than just an annoyance. It’s a signal that something inside the joint complex is struggling. For millions of people, this discomfort stems from two closely linked issues: rotator cuff injuries, which involve damage to the muscles stabilizing the shoulder, and subacromial bursitis, inflammation of the fluid-filled sac that cushions those tendons. Understanding the difference between these conditions-and how they feed into each other-is the first step toward getting your life back. You don’t need to accept chronic pain as part of aging or overuse. With the right approach, most cases resolve without surgery.
The good news? About 80% of people with rotator cuff tendinitis or bursitis see significant improvement through non-surgical methods alone. The key lies in a structured progression from immediate pain management to targeted rehabilitation. This guide breaks down exactly what’s happening in your shoulder, why standard advice sometimes fails, and the specific protocols that actually work based on current orthopedic evidence.
Understanding the Mechanics: Why Your Shoulder Hurts
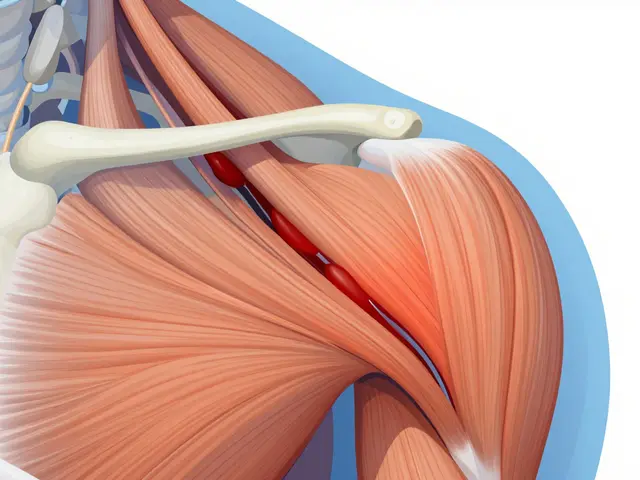
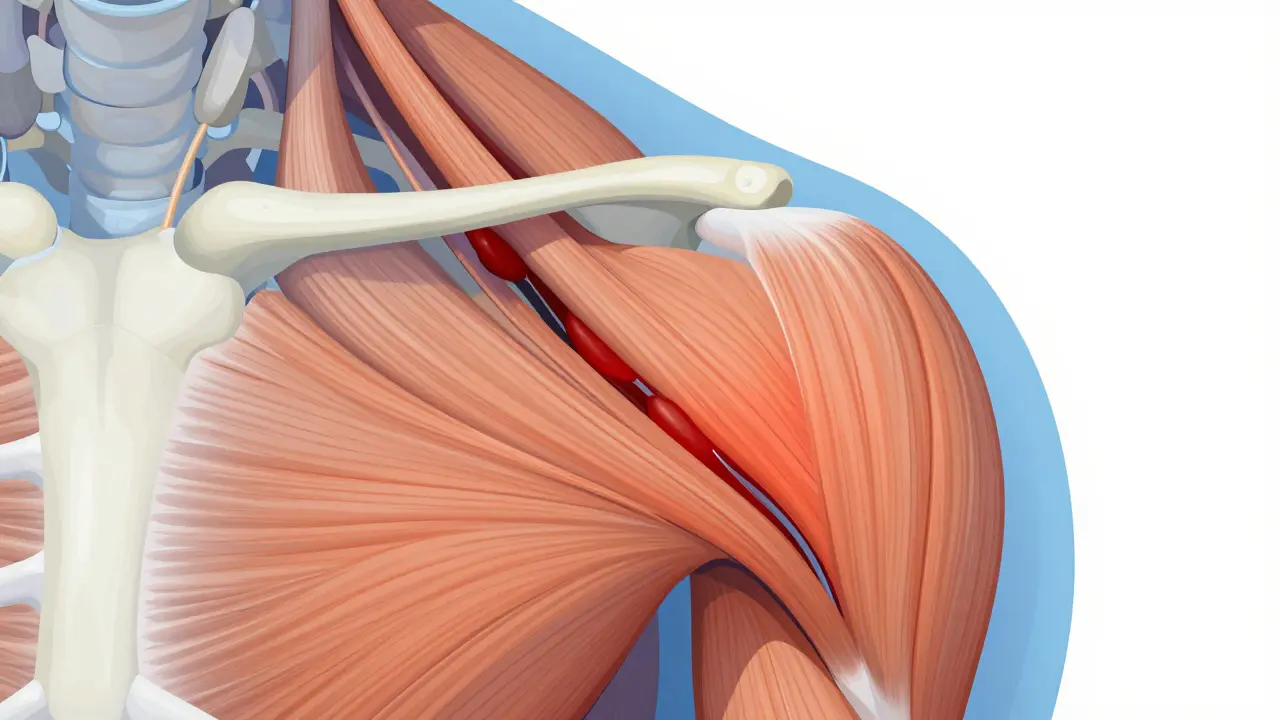
To fix the problem, you first have to understand the machinery. Your shoulder isn’t a simple ball-and-socket joint; it’s a complex assembly designed for mobility rather than stability. The rotator cuff consists of four muscles-supraspinatus, infraspinatus, teres minor, and subscapularis-that wrap around the shoulder blade and attach to the upper arm bone. Their job is to keep the head of the humerus centered in the socket while you move your arm.
Sitting right above these tendons is the subacromial bursa, a thin, fluid-filled sac about 1-2 cm thick. Think of it like a pillow that prevents friction between the rotator cuff tendons and the acromion process (the bony roof of your shoulder). When this space gets crowded-due to swelling, poor posture, or repetitive overhead motion-the bursa inflames. This is subacromial bursitis.
Here’s the catch: bursitis and rotator cuff tendinitis rarely happen in isolation. Dr. Charles Neer, who described impingement syndrome in the 1970s, showed us that when the acromion rubs against the rotator cuff during elevation, it irritates both the tendon and the bursa. This creates a vicious cycle: inflammation causes swelling, swelling reduces space, reduced space causes more rubbing, and more rubbing causes more inflammation.
You’ll likely experience a "painful arc"-sharp pain between 60° and 120° of lifting your arm away from your body. Nighttime pain is also a hallmark symptom, often waking you up if you roll onto the affected side. If you’re feeling a dull, poorly localized ache that worsens with overhead activity, you’re probably dealing with this exact mechanical conflict.
Immediate Actions: What to Do in the First Two Weeks
When the pain starts, instinct might tell you to push through it or completely immobilize the arm. Both extremes can make things worse. The goal in the acute phase (first 2-4 weeks) is to calm the inflammation without losing range of motion.
- Relative Rest: Stop the activities that trigger the pain, especially overhead movements. Don’t stop moving entirely, but avoid heavy lifting or repetitive reaching.
- Ice Therapy: Apply ice packs for 15-20 minutes, 3-4 times daily. This helps reduce the swelling in the bursa and surrounding tissues.
- Anti-Inflammatories: Nonsteroidal anti-inflammatory drugs (NSAIDs) like ibuprofen (400-600 mg three times daily) can help break the inflammation cycle. Use them as directed by your doctor, not as a long-term solution.
- Sleep Positioning: Sleep on your back or the unaffected side. If you must sleep on the painful side, hug a pillow to support the arm and prevent the shoulder from collapsing forward.
A common mistake is ignoring the "pain paradox." Some discomfort during movement is normal in the early stages, but sharp pain is a stop sign. Monitor your pain on a 0-10 scale. Keep your activity level below a 5. If it spikes higher, you’ve done too much.

The Role of Injections: Steroids vs. PRP
If conservative measures don’t bring relief after 4-6 weeks, many doctors suggest a corticosteroid injection. These injections contain triamcinolone acetonide mixed with lidocaine and are delivered directly into the subacromial space, often under ultrasound guidance. They provide rapid pain relief for 65-75% of patients, lasting 4-12 weeks. This window of relief is crucial because it allows you to participate effectively in physical therapy.
However, there are limits. The University of Utah Health recommends no more than 2-3 steroid injections per year, spaced at least 3 months apart. Frequent use can weaken tendons, increasing the risk of rupture by up to 8%.
For those seeking alternatives, Platelet-Rich Plasma (PRP) injections have emerged as a second-line option. Recent guidelines from the American Shoulder and Elbow Surgeons (March 2024) highlight PRP’s potential, citing a 68% success rate in multicenter trials compared to 52% for repeat steroid injections. While PRP doesn’t offer the immediate numbing effect of steroids, it may promote longer-term tissue healing. Discuss these options with your specialist to determine which aligns with your recovery timeline.
Rehabilitation Protocols That Actually Work
This is where most people stumble. Pain relief is temporary if you don’t fix the underlying mechanics. Physical therapy isn’t just about stretching; it’s about retraining the muscles that stabilize the shoulder blade and control the arm bone.
Dr. Scott Faucett, Director of Shoulder Surgery at MedStar Union Memorial Hospital, outlines a clear progression:
- Weeks 1-2: Pendulum Exercises. Lean forward, let the painful arm hang loose, and gently swing it in small circles. Do this for 5-10 minutes, three times daily. This maintains mobility without engaging the inflamed tendons.
- Weeks 3-4: Active-Assisted Range of Motion. Use your good arm to help lift the injured one. Focus on gentle stretching within a pain-free range.
- Weeks 4-6: Scapular Stabilization. This is critical. Squeeze your shoulder blades together (retraction) for 3 sets of 15 repetitions daily. Studies show patients focusing on scapular control recover 30% faster than those only strengthening the rotator cuff.
- Weeks 6+: Resisted Strengthening. Introduce resistance bands at 30-50% of maximum effort. Perform 15-20 repetitions per set. Focus on external rotation and abduction.
Consistency beats intensity. The AAOS recommends 2-3 therapy sessions weekly for the first month, followed by 1-2 sessions for another 4-8 weeks. But the real work happens at home. Dedicate 20-30 minutes daily to your home exercise program. Patients using smartphone apps for reminders complete 82% of their exercises, leading to 27% faster functional recovery compared to those without tracking tools.
| Approach | Time to Relief | Success Rate | Key Risks |
|---|---|---|---|
| Conservative Management (PT + NSAIDs) | 8-12 weeks | 80% | Low (<0.5% complication rate) |
| Corticosteroid Injection | 1-2 weeks | 65-75% (temporary) | Tendon weakening if overused |
| Arthroscopic Decompression | 4-6 months | Variable (modest benefit over PT alone) | Surgical risks, higher cost ($15k-$20k) |

When Surgery Becomes Necessary
Despite best efforts, some cases don’t respond to non-operative care. The American Academy of Orthopaedic Surgeons reserves surgery for patients who fail 3-6 months of comprehensive conservative treatment. The most common procedure is arthroscopic subacromial decompression, where surgeons remove a small portion of the acromion bone and inflamed bursa to create more space for the tendons.
It’s important to manage expectations here. A 2022 randomized controlled trial in the Journal of Bone and Joint Surgery found no significant difference in outcomes at 12 months between surgical and non-surgical groups for isolated bursitis. Surgery is generally more indicated for full-thickness rotator cuff tears, especially in patients under 60. For older adults with complete tears, conservative management still yields a 40% healing rate, making surgery a nuanced decision based on activity levels and pain severity.
Avoiding Recurrence: Long-Term Strategies
Getting better is only half the battle. Recurrence rates hover around 15-20%, often triggered by the "weekend warrior" phenomenon-returning to high-intensity activities before the tissue has fully adapted. To prevent this:
- Maintain Strength: Continue scapular stabilization and rotator cuff exercises 2-3 times weekly even after pain subsides.
- Check Your Posture: Forward-rounded shoulders narrow the subacromial space. Practice chest-opening stretches and ergonomic adjustments at your workstation.
- Gradual Return: Increase activity volume by no more than 10% per week. Listen to your body; mild soreness is okay, sharp pain is not.
New technologies are also helping. Wearable sensors and blood flow restriction training are emerging tools that can accelerate recovery and correct form in real-time. As the industry evolves, integrating these tools with traditional rehab may become the new standard for preventing chronic shoulder issues.
How long does it take to heal from subacromial bursitis?
Most cases of subacromial bursitis improve significantly within 8-12 weeks of consistent conservative treatment, including rest, ice, NSAIDs, and physical therapy. However, full resolution and return to high-level activities may take 3-6 months depending on severity and adherence to rehab protocols.
Is rotator cuff repair surgery always necessary for tears?
No. Approximately 80% of rotator cuff tendinitis and partial tear cases respond well to non-surgical management. Surgery is typically reserved for full-thickness tears in younger, active patients or those who fail 3-6 months of intensive physical therapy and injections.
What is the "painful arc" in shoulder pain?
The "painful arc" refers to pain experienced between 60° and 120° of shoulder abduction (lifting the arm out to the side). It occurs because the rotator cuff tendons and bursa are pinched under the acromion bone during this specific range of motion, a hallmark sign of impingement syndrome.
Can I do exercises if my shoulder hurts?
Yes, but with caution. Gentle pendulum exercises and range-of-motion movements are encouraged early on to prevent stiffness. Avoid exercises that cause sharp pain or exceed a 5/10 on the pain scale. Strengthening should only begin once acute inflammation has subsided, usually after 2-4 weeks.
How many corticosteroid injections are safe for shoulder bursitis?
Medical guidelines recommend limiting corticosteroid injections to 2-3 per year, with at least a 3-month interval between them. Excessive use can weaken the rotator cuff tendons, increasing the risk of rupture. They are intended as a bridge to enable effective physical therapy, not a standalone cure.