
Steroid Injection Risk Assessment
How Safe Are Your Injections?
Answer these questions to understand your personal risk of complications from intra-articular steroid injections based on recent medical research.
Your Risk Profile
For decades, intra-articular steroid injections have been a go-to solution for joint pain-especially from osteoarthritis. You feel it in your knee, your hip, your shoulder. The pain is sharp, constant, or worse after walking. Your doctor offers a shot. Within days, the pain fades. It feels like magic. But what if that relief comes with hidden costs? What if the injection, meant to save your joint, is quietly speeding up its breakdown?
What You’re Really Getting
Intra-articular corticosteroid injections (IACS) deliver powerful anti-inflammatory drugs directly into a joint. Common types include triamcinolone acetonide, methylprednisolone acetate, and betamethasone. Doses vary from 10 to 80 mg depending on the joint-knees get more than fingers. The idea is simple: local treatment, no system-wide fallout. But that’s not what’s happening.
Studies show steroids don’t stay put. Even when injected into a deep joint like the hip or knee, some of the drug leaks into your bloodstream. Triamcinolone acetonide, one of the most commonly used, is especially good at escaping. A 2023 study in Radiology tracked over 1,000 patients and found clear signs of systemic absorption. That means your liver, your adrenal glands, your bones-they’re all getting a dose, not just the inflamed joint.
The Hidden Damage Inside Your Joint
The biggest shock? These injections might be making your arthritis worse. It sounds backwards. You get the shot to protect your joint, but research now shows they can accelerate joint destruction.
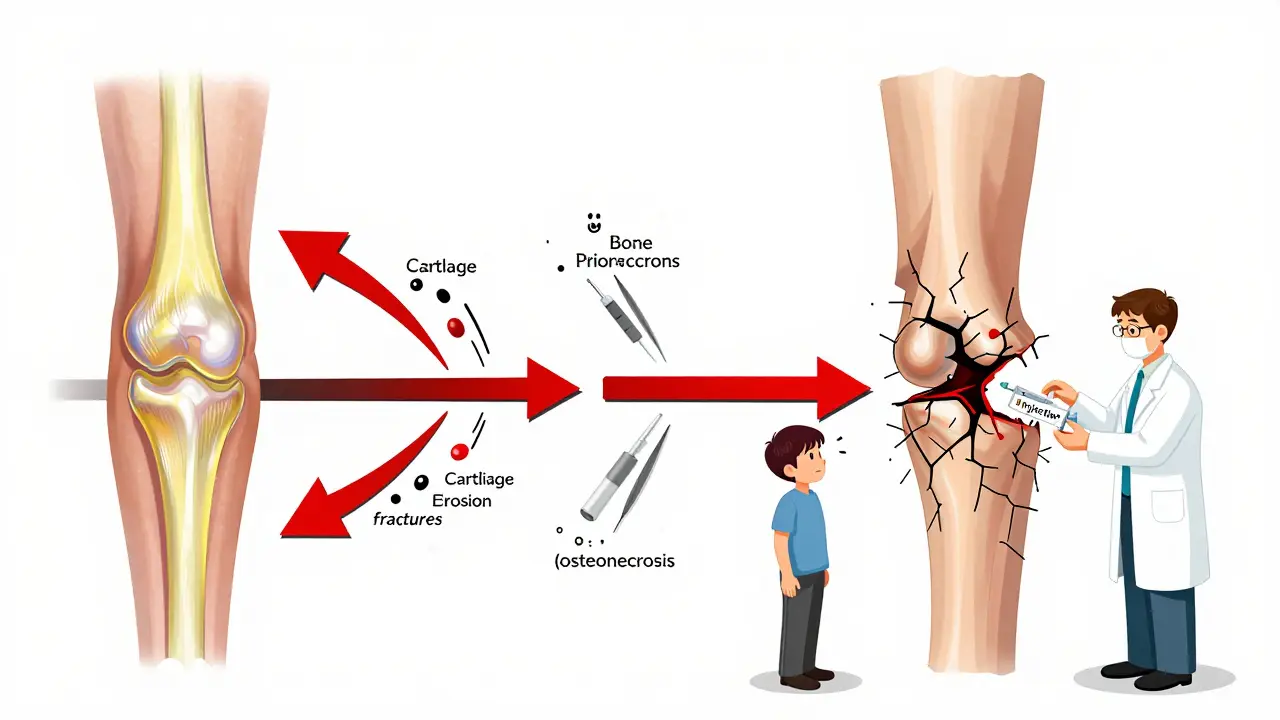
A 2023 study led by Dr. Ali Guermazi at Boston University found that patients who received corticosteroid injections had a 2 mm or greater loss of joint space over 12 months-clear evidence of cartilage erosion. This wasn’t slow, natural wear. This was rapid. In fact, patients who got repeat injections had over four times the odds of radiographic progression compared to those who didn’t get any. For hip injections, 44% of patients showed narrowing of the joint space in just six months.
It’s not just cartilage. The same study found three other serious complications: subchondral insufficiency fractures (tiny cracks under the cartilage), osteonecrosis (bone death due to poor blood flow), and rapid joint destruction. These aren’t rare. In a group of 1,000 patients, 1% developed one or more of these issues. That might sound small, but with 12 million injections given yearly in the U.S. alone, that’s 120,000 people a year at risk.
What Happens to Your Whole Body
When steroids leak into your bloodstream, they don’t just sit there. They act like a flood of artificial cortisol-your body’s natural stress hormone. This disrupts your natural balance.
Common systemic side effects include:
- High blood sugar-especially dangerous for diabetics. Blood glucose can spike within hours and stay elevated for days.
- High blood pressure-fluid retention from steroids increases pressure on blood vessels.
- Facial flushing-a temporary but noticeable redness in the face and chest.
- Adrenal suppression-your body stops making its own cortisol. This can last weeks. If you get sick or injured, your body might not respond properly.
- Osteoporosis-bone density drops. This is especially risky for postmenopausal women and older adults.
- Cushing syndrome-with repeated use, you can develop a moon face, buffalo hump, and weight gain around the midsection.
These aren’t just side effects you read about in brochures. These are real, measurable changes in your body. The American Journal of Roentgenology (2024) confirmed that even a single injection can cause adrenal suppression for up to three weeks. That’s longer than most people think.
The Debate Among Experts
Not all studies agree. Some say the risks are minimal. A 2023 NIH review found no major difference between steroid injections and placebo in terms of joint damage. Another study by Dr. Raynauld saw no joint space narrowing on X-rays. So why the confusion?
The answer lies in how you measure damage. X-rays show bone spacing, but they miss early cartilage loss. MRI scans-used in newer studies-show soft tissue breakdown before it’s visible on X-rays. That’s why Dr. Guermazi’s team used MRI: they caught damage others missed. Also, timing matters. One injection might be safe. Three in a year? That’s a different story.
Dr. McAlindon’s 2017 study showed cartilage loss over two years with repeated shots. But it didn’t show bone marrow lesions or complete cartilage loss. So yes, damage happens-but it’s not always dramatic. It’s slow. Silent. And cumulative.
Who’s at Highest Risk?
Not everyone reacts the same. Certain people face much higher risks:
- People with diabetes-steroids spike blood sugar. Repeated injections can make control harder.
- Postmenopausal women-bone density is already declining. Steroids make it worse.
- Younger patients-if you’re 45 with early osteoarthritis, you have decades ahead. Each injection adds up.
- Those with mild or no X-ray changes-if your X-ray looks fine but you’re in pain, the problem might not be arthritis. Injecting steroids here could mask something else, like a stress fracture or early infection.
- People planning surgery-steroid shots within 3-6 months of joint replacement increase infection risk and delay healing.
These aren’t just "be careful" warnings. These are red flags. If you fit even one of these categories, the risks may outweigh the short-term relief.
What Are the Official Limits?
Most guidelines say: no more than 3-4 injections per joint per year. But that’s not a hard rule-it’s a suggestion based on weak evidence. The American Academy of Physical Medicine and Rehabilitation (2018) says total glucocorticoid exposure matters. That means if you’re also taking oral prednisone, every joint shot adds to your total dose. Many doctors don’t track that.
And here’s the catch: no one tracks long-term cumulative exposure. There’s no database. No warning system. You get a shot in your knee this month, another in your shoulder next month, and your doctor doesn’t connect the dots. But your body does.
When Should You Say No?
Think twice before saying yes if:
- Your pain doesn’t match your X-ray findings
- You’ve had more than two injections in the last year
- You have diabetes, osteoporosis, or high blood pressure
- You’re under 50 and have early-stage arthritis
- You’re planning surgery in the next 6 months
Also, avoid injections if your pain flares up suddenly without a clear cause. That could be an infection, a fracture, or another condition that steroids will hide-and worsen.
What Are the Alternatives?
There are safer ways to manage joint pain:
- Physical therapy-strengthening muscles around the joint reduces pressure. Studies show it’s as effective as injections for knee osteoarthritis.
- Weight loss-losing 10 pounds reduces knee pressure by 40 pounds with every step.
- Bracing or orthotics-corrects alignment and reduces wear.
- Platelet-rich plasma (PRP)-still being studied, but shows promise for cartilage protection.
- Hyaluronic acid injections-lubricates the joint without the steroid risks. Less effective for pain relief, but safer long-term.
None of these work instantly. But they don’t destroy your joint either.
The Bottom Line
Intra-articular steroid injections aren’t evil. They’ve helped millions. But they’re not harmless. The old belief-that they’re safe because they’re local-is outdated. Science now shows they can accelerate joint damage and cause systemic harm.
If you’re older, have severe arthritis, and the pain is unbearable? A shot might still be worth it. But if you’re younger, have mild symptoms, or are otherwise healthy? You’re trading long-term joint health for short-term comfort. And that’s a deal most people don’t realize they’re making.
Ask your doctor: "What’s the evidence this will help me long-term?" and "What are the risks if I get this more than once?" If they can’t answer, get a second opinion. Your joints will thank you.

Comments
As someone from Nigeria where access to specialists is rare, I’ve seen too many patients get these shots because it’s the only option available. The relief is real, but so is the cost-especially for diabetics and postmenopausal women who don’t have the resources to monitor side effects. We need community education, not just clinical guidelines. Local clinics should be required to hand out simple infographics in local languages: ‘One shot = 3 weeks of suppressed immunity. Two shots = higher fracture risk.’ No jargon. Just facts.
And let’s be honest-most doctors aren’t malicious. They’re overwhelmed. But if we don’t systematize warnings, we’re just delaying the inevitable collapse of joint health in underserved populations. This isn’t just a medical issue. It’s a justice issue.
I’ve spoken to elders in my village who’ve had 8-10 injections over 15 years. They think it’s a cure. It’s not. It’s a bandage on a broken bone. We need to shift the narrative from ‘pain relief’ to ‘joint preservation.’
Maybe we need community health workers trained to recognize early signs of bone loss. Maybe we need mobile MRI units in rural areas. Maybe we need a national registry tracking cumulative steroid exposure. It’s expensive, yes. But so is replacing 120,000 joints a year.
I’m not anti-injection. I’m pro-awareness. Let’s stop treating symptoms and start protecting bodies.
The structural integrity of articular cartilage is not merely a function of mechanical loading; it is a dynamic equilibrium governed by chondrocyte metabolism, proteoglycan synthesis, and extracellular matrix homeostasis. Corticosteroids, by suppressing NF-κB and upregulating matrix metalloproteinases, disrupt this equilibrium at the molecular level. The 2 mm joint space narrowing observed in Guermazi’s cohort is not an artifact-it is a quantifiable biological signal of irreversible degradation.
Furthermore, the systemic absorption of triamcinolone acetonide (half-life: ~12 hours) results in prolonged glucocorticoid receptor occupancy in osteoblasts and osteoclasts, leading to uncoupled bone remodeling. This is not speculation; it is demonstrated in vitro and confirmed in longitudinal MRI studies.
The assertion that ‘steroids don’t stay local’ is not merely supported by evidence-it is empirically irrefutable. The notion that localized delivery implies localized effect is a pharmacological fallacy rooted in outdated physiology.
One must also consider the temporal dynamics: a single injection may induce transient suppression of inflammatory cytokines, but repeated exposure leads to cumulative epigenetic modulation of gene expression in synovial fibroblasts-altering long-term joint behavior even after drug clearance.
Therefore, the clinical paradigm must evolve from ‘how many injections?’ to ‘what is the total glucocorticoid burden?’ and ‘what are the non-reversible consequences?’
Glucocorticoid burden. That’s the key metric. Most docs don’t track it. Patients don’t know to ask. We need a standardized ‘steroid score’-like a cholesterol number. Every injection logged. Every oral dose counted. A running total in the EHR. If you hit 200mg cumulative in a year? Auto-flag. Auto-referral to PT. No more blind shots.
Also-PRP isn’t magic. But it’s not poisoning your bones either. Why are we still defaulting to steroids? Because it’s fast. Because insurance pays for it. Because the patient leaves happy.
It’s a system failure. Not a patient failure.
So… you’re saying the thing that makes my knee stop screaming is secretly killing it? 😭
Also, I got 3 shots last year. I’m 32. I’ve never felt better. Are you telling me I’m a lab rat now? 🤔
Also also-what if I just don’t care? I need to walk. I need to work. I need to live. Not ‘preserve cartilage for 2035’.
Just sayin’.
I’m a physical therapist in Chicago. I’ve seen patients come in after their 4th knee injection-walking with a cane, terrified of stairs. They’re shocked when I say, ‘You’ve been told to rest, but you need to move.’
It breaks my heart. They think the shot was the solution. It was a pause button. And now they’ve forgotten how to move.
PT doesn’t feel glamorous. But it’s the only thing that actually rebuilds resilience.
Also-hi, I’m from the U.S. too. We can do better.
Stop overthinking it. If your knee hurts, get the shot. If it helps, you got relief. If it breaks later, you’ll get a replacement. That’s how medicine works. You don’t get to live forever. Get over it.
This whole thing is just liberal fearmongering. Steroids are fine. My uncle got 12 shots and still runs marathons. You people need to chill. Also, I’m not diabetic so I don’t care. And why are we even talking about this? Just let doctors do their job.
I get it. The science is scary. But so is chronic pain. I’ve been living with knee OA for 8 years. I’ve tried PT, weight loss, braces. Nothing worked like the shot did.
I’m not saying this is perfect. I’m saying… sometimes you need to choose what lets you breathe today.
Maybe the answer isn’t ‘never again’-but ‘how often, and with what awareness?’
I’m not reckless. I’m realistic.
I think about how much we’ve been sold on quick fixes. Injections. Pills. Apps. Diets.
What if the real problem isn’t the joint… but the way we’ve stopped moving? Stopped listening? Stopped accepting that aging means change?
I got my first shot last year. Felt amazing. Then I cried for an hour.
Because I realized I was so desperate for relief, I didn’t ask what it cost.
Not everyone can afford PT. Not everyone has time. Not everyone has support.
So we’re left choosing between pain… and slow destruction.
Neither feels like freedom.
Let’s cut the drama. Steroids work. They’re not perfect. But neither is surgery. Or PT. Or waiting.
Doctors aren’t hiding this. They’re weighing trade-offs every day. If you’re 65 and your knee is bone-on-bone? A shot gives you 6 more months of hiking with your grandkids.
That’s not ignorance. That’s triage.
Yes, long-term risks exist. But so does loneliness. So does depression. So does giving up on life because you can’t walk to the mailbox.
Don’t shame people for choosing quality over longevity. We’re not robots. We’re humans with bad knees.
It is imperative to underscore that the purported ‘systemic absorption’ of intra-articularly administered corticosteroids is not merely a phenomenon of pharmacokinetic leakage, but a direct violation of the principle of targeted therapeutic intervention. The very foundation of localized delivery is predicated upon the assumption of minimal systemic bioavailability-an assumption now empirically invalidated by multiple peer-reviewed studies, including those employing LC-MS/MS quantification of serum corticosteroid levels.
Furthermore, the assertion that ‘1% of patients’ experience complications is statistically misleading. In a population of 12 million annual injections, 1% represents 120,000 individuals experiencing subchondral insufficiency, osteonecrosis, or adrenal crisis. This constitutes a public health crisis of epidemic proportions, yet remains unacknowledged by regulatory bodies.
One must also consider the ethical implications of informed consent: if 90% of patients are unaware of the risk of adrenal suppression lasting up to three weeks, can consent truly be informed? The current paradigm is not merely flawed-it is ethically indefensible.
My mom got her first shot at 58. Now she’s 72. Had 11. Last one was 6 months ago. She’s got a walker now. Her hips are bad. Her spine is stiff.
I wish someone had told her: ‘This isn’t a cure. It’s a delay. And delays add up.’
But no one did. Because no one knew. Or didn’t want to scare her.
Maybe the real tragedy isn’t the injection.
It’s that we never taught people how to ask the hard questions.
The American Academy of Orthopaedic Surgeons recommends no more than three injections per joint per year. The American College of Rheumatology advises caution in patients with diabetes. These are not arbitrary numbers. They are evidence-based thresholds. The issue is not the injection-it is the lack of standardized documentation and follow-up protocols.
Let us not conflate anecdotal experience with population-level risk. We must improve systems, not demonize interventions.
yeh so like steroids bad? ok but i got a shot last month and i can finally walk to my car again so idk man. also my doc never said anything about bone death. maybe they should write it on the receipt?