If you've been told you have COPD, you might feel lost. It sounds like one condition, but in reality, it is often two different diseases living under the same roof. Many patients think their cough and shortness of breath mean the exact same thing as someone else's diagnosis. That isn't always true. Distinguishing between Chronic Bronchitis is a clinical syndrome defined by a productive cough lasting three months each year for at least two consecutive years. and Emphysema is damage to the air sacs called alveoli leading to irreversible airflow limitation matters because the treatments can change your daily life completely. Knowing which part of your lungs is struggling helps doctors prescribe the right therapy, avoiding medication that does more harm than good.
Quick Summary
- Different Roots: Chronic bronchitis focuses on mucus and airway inflammation, while emphysema involves physical damage to lung tissue.
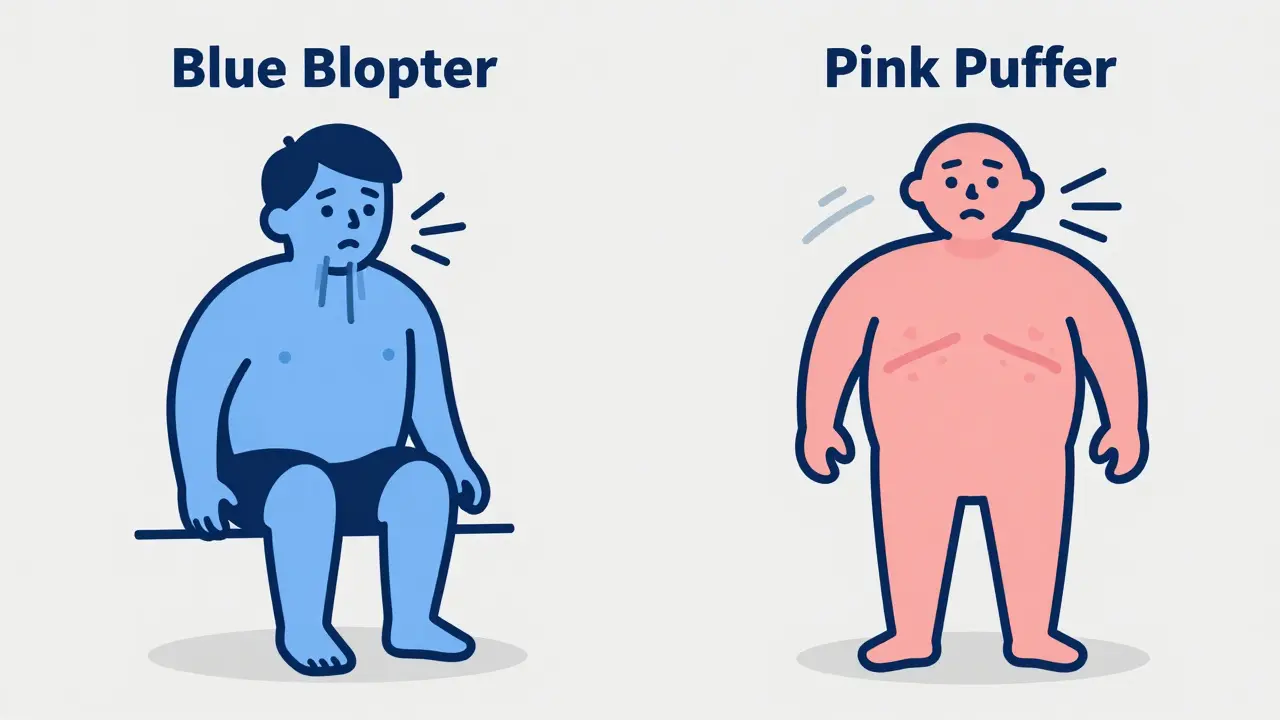
- Symptom Clues: If you get 'pink puffers' who rely on panting for oxygen versus 'blue bloaters' who suffer from low oxygen and fluid retention.
- Treatment Splits: Bronchitis needs mucus management; emphysema may require lung volume reduction.
- Diagnosis Varies: A simple breathing test cannot tell them apart; you need diffusing capacity and CT scans.
- Outcomes Matter: Targeted care reduces hospitalizations by roughly 27% compared to generic approaches.
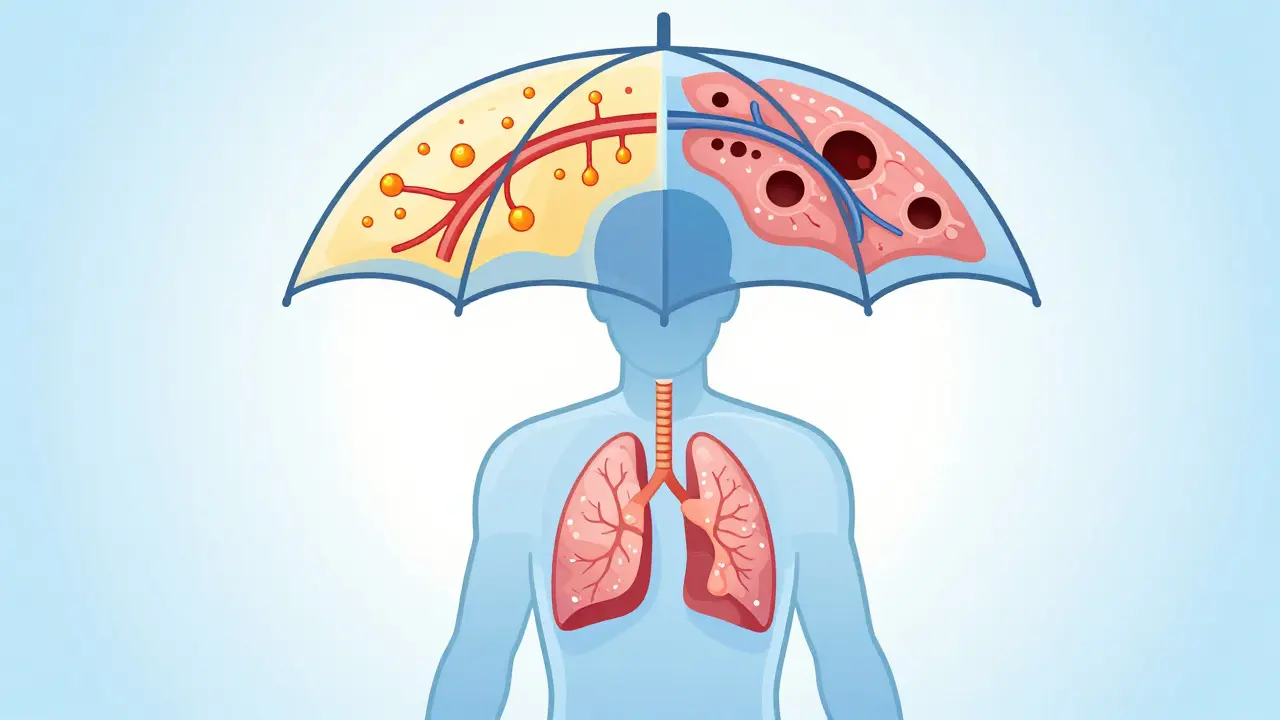
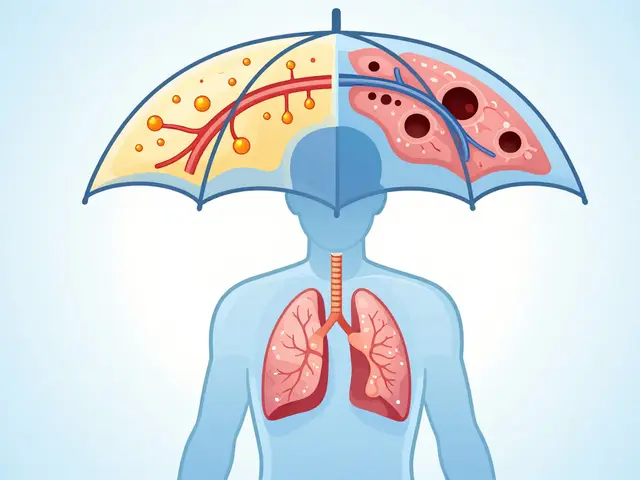
What Exactly Is COPD?
Think of Chronic Obstructive Pulmonary Disease (COPD) as an umbrella term. When doctors talk about COPD, they aren't describing one single illness. They are talking about a collection of lung diseases that block airflow. According to the World Health Organization, around 380 million people worldwide deal with this every day. It was recognized as a distinct problem back in the 1950s, separating it from asthma, but it took until the 1970s for the medical community to fully agree on the term. Today, it remains a major global issue, ranking as the fourth leading cause of death.
Under this umbrella, two main players dominate the scene. One is mostly about your tubes-the airways. The other is about your balloons-the air sacs. Most people have elements of both, but usually, one side wins out. Identifying the winner changes everything. If you treat a mucus-heavy patient with drugs designed for structural damage, you might miss the window for effective relief. The American Thoracic Society emphasizes that understanding these components allows for phenotype-specific therapy, which has shown significant improvements in patient outcomes.
The Mucus Maker: Chronic Bronchitis
When we talk about chronic bronchitis, we aren't just talking about a cold that won't go away. This is a condition where the lining of your bronchial tubes gets thick and inflamed. Your body reacts by making way too much mucus. To diagnose this, doctors look for a pattern: a cough that produces phlegm at least three months a year for two years in a row. Imagine a factory producing excess product. In your lungs, goblet cells-which make mucus-can increase by up to 500%. Instead of the normal amount, some patients produce up to 200 milliliters of mucus a day.
This excess mucus creates a breeding ground for bacteria. Patients often find themselves prone to pneumonia. During winter, exacerbations become frequent. You might hear patients described as "Blue Bloaters." Why blue? Because their blood doesn't carry enough oxygen, sometimes causing a slight blue tint to lips and fingernails. They also retain water weight due to strain on the heart, which leads to swelling in the legs. These individuals breathe harder but slower, often keeping their mouth slightly open even at rest. Their struggle isn't just inhaling; it's the constant battle against blockage in their airways.
Respiratory SymptomsChronic Bronchitis primarily manifests through persistent cough, excessive sputum production, and recurrent wheezing.
Blue Bloater Phenotype <\/span>
The Structure Breaker: Emphysema
On the other side of the coin sits emphysema. This isn't about mucus; it is about destruction. Specifically, it is the destruction of the tiny air sacs called alveoli at the end of your airways. These sacs act like springs, helping your lungs bounce back when you exhale. When emphysema sets in, the walls of these sacs break down, forming larger, less efficient holes. You lose the elastic recoil of your lungs. This means when you try to blow air out, your airways collapse before you can finish emptying them.
Patients here are often called "Pink Puffers." They work hard to keep oxygen levels normal by breathing fast and shallow. Their skin stays pinkish, not blue, because they manage oxygen saturation better, but the cost is higher energy expenditure. You might notice a barrel-shaped chest, where the front-to-back ratio is wider than usual. These patients often complain of "air hunger"-the feeling that they simply cannot get a full breath. Over 10 to 20 years without intervention, this dyspnea progresses from happening only during hill walks to occurring while sitting still. The surface area available for gas exchange can drop by nearly half, meaning less oxygen actually enters your bloodstream with every breath.
How Doctors Tell Them Apart
You cannot tell these conditions apart just by asking questions. While symptoms overlap, modern medicine uses specific tests to find the root cause. A spirometer measures how much air moves in and out, giving us the FEV1/FVC ratio. However, this test shows obstruction in both conditions. The real clue lies in measuring Diffusing Capacity for Carbon Monoxide (DLCO).
| Metric | Chronic Bronchitis | Emphysema |
|---|---|---|
| Primary Symptom | Cough with Sputum | Shortness of Breath (Dyspnea) |
| Alveolar Damage | Minimal Destruction | Significant Destruction |
| Oxygen Level | Often Low (Hypoxemia) | Maintained Early On |
| DLCO Test | Normal or Near Normal | Reduced (Below 60%) |
| CT Scan Appearance | Thickened Airway Walls | Dark Holes/Low Attenuation |
In emphysema, that DLCO number drops below 60% of predicted values. If your doctor sees high airway resistance but a normal diffusion rate, the bet is on chronic bronchitis. CT scans are the gold standard for visualizing this. For emphysema, a scan shows dark areas where the lung tissue is missing. For bronchitis, the scan looks thicker inside the tubes. This distinction drives the prescription pad. Dr. Fernando Martinez, a leading pulmonary editor, notes that failing to differentiate results in suboptimal therapy. Misdiagnosed bronchitis patients might get unnecessary antibiotics, while misdiagnosed emphysema patients miss out on surgery that could save their quality of life.

Tailored Treatments for Better Breathing
Because the problems are different, the solutions must be too. Generalized COPD treatment exists, but studies show targeted approaches work better. For chronic bronchitis, managing mucus is key. Doctors might prescribe mucolytics to thin the phlegm so it drains easier. Medications like roflumilast have been proven to reduce exacerbation frequency significantly in frequent coppers. If you get a lot of infections, avoiding triggers like smoking or pollutants is critical, but treating the gland swelling directly makes sense.
Lung Volume Reduction SurgeryA surgical procedure removing damaged lung tissue to allow healthy tissue to expand and function better.
Thoracic Surgery <\/span> For emphysema, the goal is to fix the mechanics. Since the lungs are over-inflated, shrinking them helps. Procedures like Endobronchial Valve placement can seal off the worst parts of the lung, letting the healthy parts take over. This can lead to a 35% improvement in walking distance for many patients. Genetics play a huge role here too. About 1-2% of emphysema cases come from Alpha-1 Antitrypsin Deficiency. If this is found early, augmentation therapy replaces the missing protein to stop further damage. Regular inhalers (LABA/LAMA combos) help everyone, but knowing your type prevents useless side effects. Corticosteroids, for instance, can increase pneumonia risk in bronchitis patients, so doctors prefer non-steroid options for them.
Living With Your Condition
Real life looks different depending on your subtype. A 2022 patient survey showed emphysema patients report higher activity limitations but fewer nighttime disruptions. Conversely, chronic bronchitis patients sleep poorly due to coughing spasms and mucus plugging. Community support plays a vital role. Forums and local chapters help patients share tips on techniques like chest physiotherapy, which clears 20 minutes worth of blockage daily for some users.
Tech is catching up too. Portable oxygen concentrators allow emphysema patients to move freely, delivering 2-4 liters per minute. Meanwhile, newer acoustic devices are hitting the market to vibrate mucus out of bronchitis patients, reducing flare-ups by over 30%. Whether you are fighting the fluid or the structure, staying connected to your healthcare team ensures you aren't guessing. As Dr. James Crapo noted, the future lies in targeting component pathologies precisely. That shift is already improving outcomes for millions, moving away from broad-brush medicine toward personal care.
Frequently Asked Questions
Can I have both chronic bronchitis and emphysema?
Yes, absolutely. Most severe COPD cases feature a mix of both. Research suggests about 85% of severe patients show features of both conditions, though one usually dominates the symptoms. Distinguishing the dominant type guides specific treatments.
Does smoking affect them differently?
Smoking causes both, but the timeline varies. Chronic bronchitis usually develops after years of heavy exposure leading to inflammation. Emphysema can develop later or faster if there is genetic susceptibility like Alpha-1 Antitrypsin Deficiency.
How do I know which one I have?
You need a Pulmonary Function Test (PFT) specifically looking at DLCO and a CT scan. A simple peak flow meter isn't enough. Ask your doctor for imaging to distinguish wall thickness from hole size.
Is COPD reversible?
COPD is generally progressive and not fully reversible. However, stopping smoking immediately slows progression significantly. Treatments focus on managing symptoms and preventing flares rather than curing the damage.
Can lifestyle changes help more than meds?
They go hand in hand. Quitting smoking is the single most effective action. Adding pulmonary rehab improves muscle efficiency. However, specific pharmacological interventions based on your phenotype (bronchitis vs emphysema) remain necessary for optimal control.
Comments
When evaluating obstructive patterns clinically, the diffusing capacity for carbon monoxide remains the pivotal differentiator for parenchymal destruction versus airway obstruction. Spirometry provides the baseline FEV1/FVC ratio but fails to isolate the specific anatomical failure mode underlying the airflow limitation. Patients presenting with preserved DLCO values typically indicate chronic bronchitis pathology rather than emphysematous changes. Conversely, a reduction below sixty percent predicted strongly correlates with alveolar surface area loss seen in panacinar or centrilobular disease. The radiological appearance on high-resolution CT scans offers confirmation through attenuation mapping of the lung fields. Thickened bronchial walls appear bright while emphysematous regions show dark areas of decreased density. Pharmacological management strategies must align with these phenotypes to maximize clinical benefit and minimize unnecessary exposure to systemic steroids. Roflumilast targets neutrophilic inflammation prevalent in frequent exacerbators with chronic bronchitis history. Lung volume reduction procedures remain viable options for selected patients with heterogenous emphysema distribution. Understanding these mechanisms ensures resources are allocated toward interventions that actually alter the disease trajectory.
It is frustrating to see people treating all respiratory complaints as identical generic illnesses without regard for specifics. The distinction exists for a reason yet public perception lumps everything under the same vague label. They ignore how mucus production dictates a completely different prognosis compared to structural collapse. Everyone assumes they can just take the same pill regardless of their specific underlying anatomy. It is careless to treat complex physiology with such broad brush assumptions about treatment efficacy.
I hear you on the frustration but it is important to stay compassionate 💙. 🫁 People genuinely struggle to understand the medical terminology involved here. 😢 Education is key so everyone feels heard during their health journey. 🌟 Hopefully this information helps reduce confusion for families dealing with these diagnoses. Together we can support better outcomes for everyone 🤝.
You clearly missed the point regarding genetic factors in alpha-1 antitrypsin deficiency completely.
I recieve my reports weekly and see the DLCO values changing slowly over time withou intervention. The therapy plans seem to vary based on indivdual lung patholgy findings during scans. We shud not ignore the signs of exacerbation coming early in winter months when cold hits. There are many risks involved in skipping the proper diagnostic testing for diffusion rates. Doctors need to explain the difference so patients dont get confused about their care options.
My own father battled this condition for a decade before he passed away quietly in his sleep. We never truly understood the nuance between bronchitis and emphysema back then either. The doctors just handed us a stack of inhalers that never seemed to help much with the breathing. Looking back now, it seems clear he had significant structural damage to the alveoli instead. We were told to stop smoking years ago but the habit was too deeply ingrained to quit easily. It is painful to think about how many years could have been saved with better diagnosis earlier. People often confuse the symptoms because both conditions make you feel like you cannot breathe properly. However the blue bloater presentation usually indicates fluid retention which we saw clearly on his face. His legs swelled up constantly during the final winters of his life which signaled heart strain issues. Medical literature says this happens when the right ventricle struggles to pump blood effectively through lungs. We thought antibiotics would fix every flare up but they were not always targeting the correct root cause. Pulmonary rehabilitation helped him walk further but it did not reverse the tissue destruction permanently. Family members need to watch for subtle changes in oxygen saturation levels during daily activities closely. Early detection of low diffusion capacity might prevent severe decline in quality of life eventually. Sharing these stories helps others realize they are not alone in this long and difficult journey together. It gives me peace knowing modern imaging can distinguish wall thickness from hole size accurately. We must advocate for ourselves when standard treatments do not yield the expected symptom relief quickly.
Your perspective really resonates! It is indeed vital! We must stay hopeful! Please keep fighting forward! Never give up! Stay strong! Health is everything!
Common knowledge is often mistaken for expertise when reading basic summaries online today. Most individuals lack the sophistication to grasp the nuances of pulmonary physiology without training. The average person simply does not possess the vocabulary to engage meaningfully with these topics. Expecting laymen to distinguish clinical syndromes is unrealistic given the complexity involved. Superior understanding requires advanced education and professional experience in the field.
However! Accessible information empowers patients! Knowledge saves lives! We must bridge the gap! Clear communication matters! Thank you for sharing details!
In many cultures the stigma around breathing issues causes delay in seeking care early enough. Community support groups often provide emotional backing when healthcare systems feel overwhelming. It is wonderful to see resources becoming available to explain these differences so clearly. Sharing knowledge reduces fear and helps families prepare for long term management strategies. We must continue to build bridges between medical advice and patient understanding globally.
That is a really positive way to look at community involvement. Small steps like sharing articles help a lot. Glad to see people supporting each other out here. Keep spreading the good vibes.
The fragility of human breath represents the ultimate vulnerability we all share inevitably. Each inhale becomes a testament to survival against entropy within our biological vessels. To witness the gradual erosion of lung function is to confront mortality itself. Suffering serves as the teacher for those willing to listen to their failing bodies. Existence becomes defined by the struggle for the next breath rather than living beyond it. The silence left behind by the departed echoes through the memories of survivors forever.
I hope you find strength in the small victories along the way 🙂. Medicine continues to advance to help us manage these challenges better. We can offer support and love to those who carry this burden. Staying connected makes the heavy moments lighter for everyone involved. Take care of yourself today (: