Autoimmune hepatitis isn't something you hear about often, but if you're living with it, you know how life-changing it can be. It’s not caused by alcohol, viruses, or fatty foods. Instead, your own immune system turns against your liver, attacking it like an invader. This leads to inflammation, scarring, and eventually, liver failure if left untreated. The good news? We know how to stop it. The challenge? The treatment isn’t simple, and the side effects can be just as hard to deal with as the disease itself.
How Is Autoimmune Hepatitis Diagnosed?
There’s no single blood test that says, "Yes, you have autoimmune hepatitis." Doctors have to piece together clues - like a detective. First, they rule out everything else: hepatitis B and C, alcohol use, fatty liver, and other autoimmune conditions. Then they look at three big things: blood markers, antibodies, and a liver biopsy.
Blood tests usually show high levels of liver enzymes - ALT and AST - often five to ten times above normal. IgG, a type of antibody, is also elevated, usually more than 1.5 times the upper limit. But the real telltale signs come from autoantibodies. About 80% of cases show antinuclear antibodies (ANA) or smooth muscle antibodies (SMA). The rest may have LKM1 antibodies, which point to a rarer subtype. Still, as of the 2025 European guidelines, these subtypes don’t change how you’re treated. That’s a big shift from just a few years ago.
The gold standard for diagnosis? A liver biopsy. It’s not fun, but it’s necessary. The biopsy looks for interface hepatitis - a specific pattern where immune cells creep into the liver tissue at the border between the portal area and liver cells. This pattern is almost unique to autoimmune hepatitis. Experts now recommend at least 20 portal tracts be examined to be sure. Without this, you’re guessing. And guessing with liver disease is dangerous.
Doctors use a scoring system - the Revised International Autoimmune Hepatitis Group (IAIHG) score - to put it all together. Points add up for abnormal blood tests, autoantibodies, liver findings, and the absence of other causes. A score over 15 means probable autoimmune hepatitis. Over 20? That’s definite. This system isn’t perfect, but it’s the best we have.
Why Steroids Are the First Line of Defense
When the immune system attacks your liver, you need to shut it down. That’s where corticosteroids come in. Prednisone (or its cousin prednisolone) is the go-to drug. It’s powerful, fast, and effective. In fact, about 80 to 90% of patients show improvement within two weeks. That’s unusually quick for an autoimmune disease.
The standard starting dose? Between 0.5 and 1 mg per kilogram of body weight - up to 60 mg a day. For someone weighing 70 kg, that’s about 35 to 70 mg daily. The goal isn’t to stay on this dose forever. It’s to get the inflammation under control as fast as possible, then taper down. By week 8, most patients are down to 10 to 15 mg a day.
But here’s the catch: steroids have a long list of side effects. Moon face. Weight gain. Insomnia. Mood swings. Bone thinning. High blood sugar. These aren’t just inconveniences - they’re serious. One patient on Reddit described gaining 30 pounds of fluid in three weeks. Another said the moon face made her feel unrecognizable. These aren’t rare stories. Up to 70% of people on steroid-only treatment develop noticeable side effects.
That’s why doctors don’t leave you on steroids alone for long.
The Role of Azathioprine - The Steroid-Sparing Partner
Azathioprine (brand name Imuran, or generic azathioprine) isn’t a miracle drug. But it’s the best partner prednisone has ever had. It doesn’t work fast. It takes weeks, sometimes months, to kick in. But it does one critical thing: it lets you cut your steroid dose by 70 to 80% within six months.
The combination is simple: start with prednisone and add azathioprine at 50 mg a day, then increase to 1 to 2 mg per kg daily - max 150 mg. It’s usually taken once a day. The magic? You get the same immune control with far fewer side effects. Only about 30% of patients on combination therapy develop serious steroid issues, compared to 70% on steroids alone.
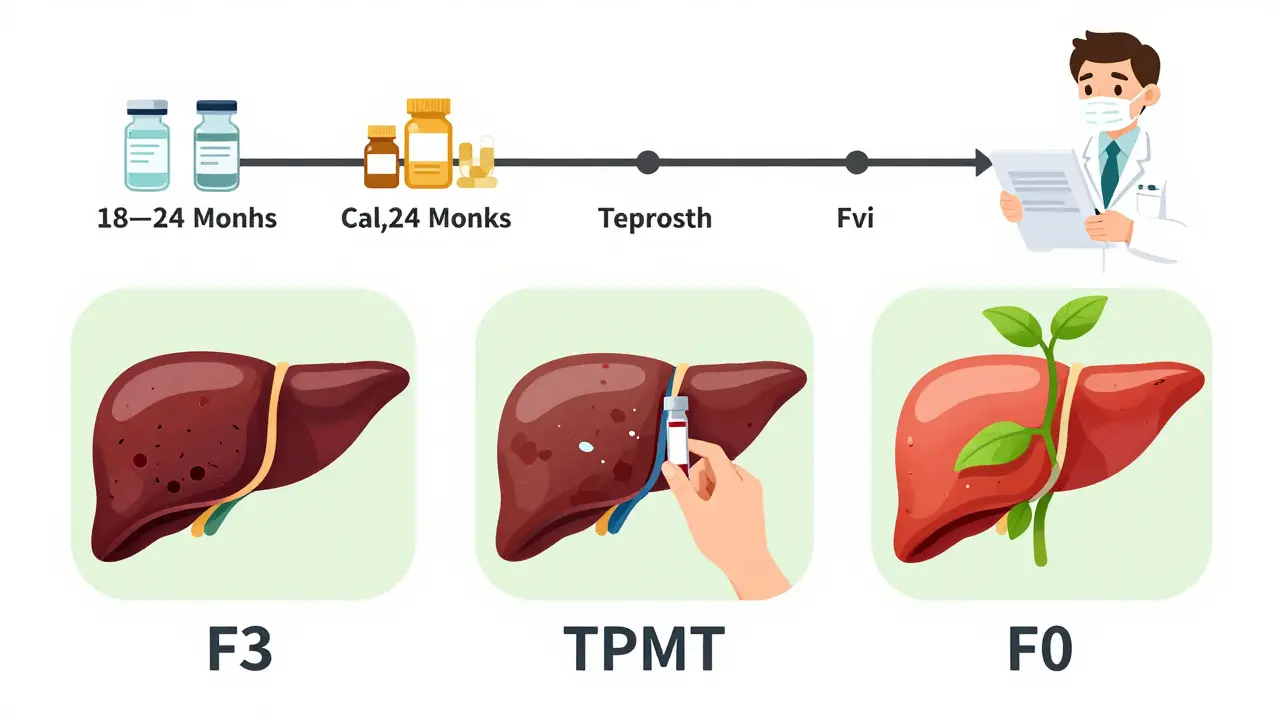
But azathioprine isn’t without risks. It can cause nausea, vomiting, and pancreatitis. In rare cases, it crashes your bone marrow, leading to dangerously low white blood cells. That’s why testing for TPMT enzyme levels is now standard before starting. About 0.3% of people have a complete deficiency - and if they take azathioprine, they could die. Testing costs $250 to $400 in the U.S., and while 78% of European centers do it routinely, only 45% of U.S. centers still do. That gap is dangerous.
Some patients can’t tolerate azathioprine at all. One user on the American Liver Foundation forum shared that 100 mg triggered pancreatitis. They switched to mycophenolate - and finally got relief after 18 months of trial and error. That’s not unusual. About 10 to 15% of patients don’t respond to first-line therapy and need second-line options.
What Success Looks Like - And When It’s Not Enough
Success isn’t just about feeling better. It’s about numbers. Complete biochemical response means ALT and AST levels return to normal, and IgG drops back into the normal range. That happens in 60 to 80% of patients within 18 to 24 months. Histological remission - meaning the liver tissue actually heals - is seen in 50 to 70% after two to three years. Some patients even reverse fibrosis, going from stage F3 (advanced scarring) to F0 (no scarring).
But remission doesn’t mean cure. About 60 to 80% of patients need lifelong maintenance therapy. If you stop treatment, relapse rates are 50 to 90%. That’s why doctors don’t rush to stop meds. Even if your blood tests look perfect, a repeat biopsy after two years is often recommended to confirm healing. Only then, and only under close supervision, might a slow taper be considered.
And even then, 70% of relapses happen within three months of stopping. So if you’re thinking about quitting, talk to your doctor first. Don’t make that decision alone.
What Happens When First-Line Treatment Fails?
Not everyone responds. About 10 to 15% of patients don’t improve after 12 to 18 months. For them, the options are limited but growing.
Mycophenolate mofetil (CellCept) is now the most common second-line drug. It’s taken twice daily, and studies show it works in about 60% of steroid-resistant cases. It’s also less toxic to bone marrow than azathioprine, which makes it a good choice for those who can’t tolerate it.
Calcineurin inhibitors like cyclosporine or tacrolimus are another option. They’re powerful, but they can damage kidneys. So they’re usually reserved for short-term use or when other drugs fail.
New hope is on the horizon. A drug called obeticholic acid (Ocaliva), originally for another liver disease, is now in phase 3 trials for autoimmune hepatitis. Early results show a 42% complete response rate - better than standard therapy. JAK inhibitors like tofacitinib and monoclonal antibodies targeting interleukin-6 are also showing promise in early trials. These aren’t available yet, but they’re coming fast.
What You Need to Know Before Starting Treatment
Before you even take your first pill, there are critical steps:
- Test for hepatitis B. If you have a past infection (even if you’re cleared), immunosuppressants can reactivate it. That can be deadly. You’ll need antiviral prophylaxis if you test positive.
- Get vaccinated. Hepatitis A and B vaccines are essential - but they only work at 40-60% effectiveness if you’re already on immunosuppressants. Get them before treatment starts.
- Do the TPMT test. It’s not optional. If you have the deficiency, azathioprine can kill you. Ask your doctor if they’ve done it. If they haven’t, push for it.
- Plan for bone health. Start calcium and vitamin D supplements. Ask about a bone density scan. Steroids thin your bones - and that damage can be permanent.
Monitoring is just as important as starting treatment. Blood tests every 2 to 4 weeks at first. Then every 3 months. IgG levels checked quarterly. Liver biopsies at 18 to 24 months. This isn’t optional. Skipping tests means you’re flying blind.
The Real Cost - Financial and Emotional
Prednisone? Generic costs $4 to $15 a month. Azathioprine? Generic is $25 to $50. But branded Imuran? $300 to $500. Mycophenolate? $800 to $1,200. Insurance helps, but not everyone has good coverage. And if you need to switch drugs? You’re looking at months of trial and error - and lost time.
Emotionally, it’s brutal. The weight gain. The mood swings. The hair loss. The fear that the treatment is worse than the disease. A 2024 patient survey found 65% of people felt steroid side effects were worse than their symptoms. Adherence rates for combination therapy? Only 75%. For monotherapy? Just 55%. That’s not laziness - it’s survival. People drop out because they can’t handle it.
But there’s hope. One patient on HealthUnlocked wrote: "After two years on 5 mg prednisone and 75 mg azathioprine, my biopsy showed complete fibrosis reversal from F3 to F0." That’s not fantasy. It’s real. And it’s why we keep fighting.
What’s Next for Autoimmune Hepatitis?
The 2025 EASL guidelines are a turning point. They dropped autoantibody-based typing. They extended the treatment response window to 6 to 12 months. They pushed for TPMT testing. They made biopsy timing clearer. These aren’t just updates - they’re better care.
Research is accelerating. Blood tests that predict steroid response within two weeks? In development. Genetic markers that identify high-risk patients? Already identified. Personalized treatment plans based on your DNA? Coming soon.
One thing is certain: autoimmune hepatitis is no longer a mystery. We know how to treat it. We know how to monitor it. We know how to prevent complications. The hardest part? Living with the treatment. But with better drugs, better testing, and better support, that’s changing too.
Comments
I was on prednisone for 8 months and honestly? It felt like living in a horror movie. Moon face, insomnia, mood swings - I cried over spilled milk. But when I added azathioprine? Life changed. I dropped from 60mg to 10mg in 4 months. My skin stopped looking like a puffed-up balloon. Still taking it 2 years later. No relapse. You can do this.
This post is FIRE 🔥. I’ve been through the wringer - biopsy, steroids, TPMT test, panic attacks over bloodwork. But here’s the truth: if you don’t push for that TPMT test, you’re playing Russian roulette with your liver. Stop waiting for your doc to bring it up. ASK. Demand it. Your life isn’t a suggestion box.
Let me guess - you’re one of those people who think 'autoimmune' means 'not real'. Wake up. Big Pharma is pushing steroids because they’re cheap and profitable. Azathioprine? They don’t make money on generics. That’s why they downplay TPMT testing. And don’t get me started on how the FDA ignores the 45% U.S. non-compliance rate. This isn’t medicine. It’s a cash grab wrapped in a white coat.
I just want to say - to anyone reading this and feeling alone - you’re not. I’ve been on this journey for 5 years. Some days I hated my reflection. Some days I wanted to quit. But I didn’t. And now? My liver biopsy came back F0. I’m not cured. But I’m alive. And I’m proud. You’re stronger than you think. 💛
Prednisone turned me into a greasy, grumpy, moon-faced gremlin. Azathioprine? The quiet hero. Took 3 months to kick in, but once it did? I got my sleep back. My energy. My damn sanity. I still have to take it daily. I still get blood drawn every 3 months. But I’m not dying. I’m living. And that’s the win.
I lost 17 pounds of muscle because my body was too busy fighting the meds to rebuild itself. I cried in the shower every morning. My husband said I looked like a ghost. I thought I’d never be me again. But I am. Slowly. Painfully. I still take 5mg of prednisone. I still have bad days. But I also have coffee on the porch. And that counts. 🫶
In India, we don’t have access to TPMT testing or even generic azathioprine in rural areas. Steroids are the only option. We watch our patients develop osteoporosis at 35. We watch them die from reactivated HBV because no one screened them. This isn’t just a medical issue - it’s a global injustice. Why do rich countries get personalized medicine while we beg for basic care? #HealthEquity
The Revised IAIHG scoring system is robust, but its application varies widely across institutions. A 2023 multicenter study found inter-observer variability in biopsy interpretation exceeding 32% when fewer than 20 portal tracts were assessed. This underscores the necessity for standardized histopathological training. Furthermore, the 2025 EASL guidelines’ recommendation to delay biopsy until after biochemical response is inconsistent with emerging data on fibrosis reversal. Clinical practice must evolve beyond protocol adherence.